What is the most accurate diagnostic tool for endometrial hyperplasia?
The most useful tool to assess endometrium and make preliminary diagnosis is ultrasound imaging (USG TV). Tissue sampling should be performed in women with risk factors of EC, who present symptoms of abnormal vaginal bleeding or pathological vaginal discharge.
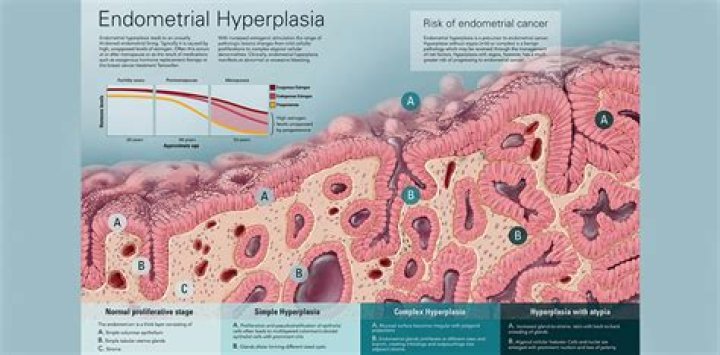
What is the difference between simple and complex endometrial hyperplasia?
Simple hyperplasia: The endometrium contains an increased number of dilatated glands. Complex hyperplasia without atypia: The glands appear crowded and are surrounded by relatively scant stroma. The glandular epithelium are lined by uniform cells, which show no nuclear atypia.
How is complex endometrial hyperplasia treated?
Endometrial hyperplasia treatment The most common treatment is progestin. This can be taken in several forms, including pill, shot, vaginal cream, or intrauterine device. Atypical types of endometrial hyperplasia, especially complex, increase your risk of getting cancer.
How do you test for endometrial hyperplasia?
A transvaginal ultrasound exam may be done to measure the thickness of the endometrium. For this test, a small device is placed in your vagina. Sound waves from the device are converted into images of the pelvic organs. If the endometrium is thick, it may mean that endometrial hyperplasia is present.
What is the treatment for simple hyperplasia without atypia?
What should the first-line medical treatment of hyperplasia without atypia be? Both continuous oral and local intrauterine (levonorgestrel-releasing intrauterine system [LNG-IUS]) progestogens are effective in achieving regression of endometrial hyperplasia without atypia.
How serious is complex atypical hyperplasia?
Simple or complex atypical endometrial hyperplasia: An overgrowth of abnormal cells causes this precancerous condition. Without treatment, your risk of endometrial or uterine cancer increases.
Can complex hyperplasia go away?
If left undiagnosed and untreated, endometrial hyperplasia will usually not abate on its own. Endometrial hyperplasia is often discovered because of abnormal uterine bleeding either between periods or after menopause.
How serious is endometrial hyperplasia?
Endometrial hyperplasia thickens the uterus lining, causing heavy or abnormal bleeding. Atypical endometrial hyperplasia raises the risk of endometrial cancer and uterine cancer. The condition tends to occur during or after menopause.
Is endometrial hyperplasia painful?
It is not fully understood why some people experience symptoms of endometrial hyperplasia, while others do not. When endometrial hyperplasia symptoms occur, they usually involve pain during intercourse or various abnormalities of menstruation, including: Heavy menstruation. Bleeding between period or after menopause.
Does simple hyperplasia go away?
Simple Hyperplasia can go away on its own or with hormonal treatment. Endometrial Hyperplasia is caused by either too much estrogen or not enough progesterone.
Can simple hyperplasia be cured?
Simple endometrial hyperplasia (without atypia): This type of endometrial hyperplasia has normal-looking cells that aren’t likely to become cancerous. This condition may improve without treatment. Hormone therapy helps in some cases.
What is endometrial hyperplasia and how is it treated?
Endometrial hyperplasia is a condition that causes abnormal uterine bleeding. These symptoms can be uncomfortable and disruptive. Many women find relief through progestin hormone treatments. Women who have atypical endometrial hyperplasia have a higher risk of developing uterine cancer.
Can atypical endometrial hyperplasia become cancerous?
Untreated atypical endometrial hyperplasia can become cancerous. Endometrial or uterine cancer develops in about 8% of women with untreated simple atypical endometrial hyperplasia. Close to 30% of women with complex atypical endometrial hyperplasia who don’t get treatment develop cancer.
What is endendometrial hyperplasia (ENH)?
Endometrial hyperplasia is a heterogeneous set of pathologic lesions that range from mild, reversible glandular proliferations to direct cancer precursors.
Why do cigc surgeons not perform open hysterectomies for endometrial hyperplasia?
Increased surgical volume is important to develop and maintain surgical expertise. CIGC surgeons do not perform open hysterectomies on patients with endometrial hyperplasia. Open surgeries are known to be painful, have a relatively high risk of complications, and have an extended recovery period.